

Difficulties in diagnosing the disease "Lung cancer"

Patient K., 37 years old.
The patient has been seen in the clinic since January 1990
· The main complaint at the time of admission to the clinic is intense headaches, observation by a therapist and a neurologist.
· From the anamnesis it is known that in childhood there was a spinal injury in the neck.
· MRI shows signs of C1 and C2 fracture with displacement of fragments, at this level - signs of narrowing of the spinal canal.
1999 to 2013
· Observation by a dentist and a neurologist.
· Data on laboratory and instrumental studies in the history of the disease are not presented.
2013
· The first visit to an endocrinologist with complaints of weakness, dry mouth, discomfort in the neck.
· On palpation, the thyroid gland is not enlarged, of a dense consistency, heterogeneous, the nodes are not palpable.
· Diagnosis - "Autoimmune thyroiditis".
Complete blood count from 18.04.2013

From 2013 to 2016
· One visit to a neurologist and a therapist for severe headache.
· An X-ray examination of the spine was performed, without dynamics.
April 2016
Contacting a therapist:
· Complaints: cough with hard-to-separate transparent sputum, palpitations, feeling of incomplete inhalation, weakness, sweating.
· Diagnosis: acute respiratory viral infection.
· Examination within the framework of MES, additionally - ECG.
Return visit to therapist
Acute respiratory viral infection, course?
Acute pharyngitis, current?
VSD cardiac type, worsening?
In May 2016, childbirth.
After giving birth, she lost 7 kg (compared to her weight before pregnancy). Since May 2017, the weight has not decreased. Since May 2017 BMI: 17.31 kg / m2 2 .
Complete blood count (dynamics).

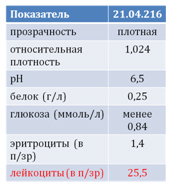
General urinalysis.
January 2017
Seeing a therapist: complaints of discomfort in the upper abdomen, decreased appetite, dry cough, palpitations.
Diagnosis:
· chronic parenchymal pancreatitis in the acute stage?
· DWP in the acute stage?
· rhythm disturbance?
· acute tracheitis (antibacterial therapy was prescribed for acute tracheitis).
Next hit: June 2017
Complaints of dry cough and herpetic eruptions on the wings of the nose.
Deterioration of health within a week.
Diagnosis: acute tracheitis.
Consultation with a pulmonologist
Complaints of dry cough, aggravated by talking, lying down, going out into a cold room.
Cough since December 2016, body temperature did not rise.
An examination was scheduled.
External respiration function:
· on the initial spirogram there is a slight decrease in VC. The patency of the bronchial tree is not impaired;
· after inhalation of a bronchodilator (Ventolin 2 doses) FEV1 decreased by 3% (paradoxical reaction);
The test is paradoxical.
Repeated consultation of the pulmonologist based on the examination results.
· Taking into account the decrease in hemoglobin over time, weight loss over time, long-term persistence of cough and preservation of accelerated ESR, it is recommended to take an X-ray of the lungs.
· A direction has been formed.
Chest X-ray (13.06.2017).
Conclusion: left-sided upper lobe pneumonia.
Provisional diagnosis:
Community-acquired bronchopneumonia in the upper lobe of the left lung -?
Pulmonary tuberculosis - ?
Follow-up plan:
CRB
Diaskintest
the sensitivity is 85% and the specificity is 99%.
Mantoux test
the sensitivity is 100% and the specificity is 75%.
T-SPOT
the sensitivity is 100% and the specificity is 98.8%.
Complete blood count, dynamics.

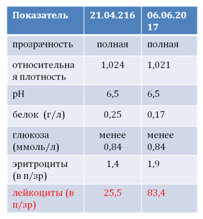
General urine analysis, dynamics.
Consultation
The chronological connection of the cough history and the detection of a darkening in the lungs with a childbirth that took place a year ago may indicate a cystic drift - chorionepithelioma.
Consultation of an oncologist and a gynecologist is required.
The second most important may be eosinophilic infiltration, as a manifestation of allergy to a stray dog living in a family, picked up on the street 2 years ago, undergoing treatment for ticks.
Consultation with an allergist is required.
The third cause of cough may be gastrobronchial reflux with the addition of banal pneumonia. For diagnostic and therapeutic purposes (ex uvantibus), prescribe Pantoprazole or Rabeprazole.
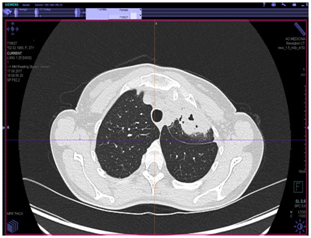
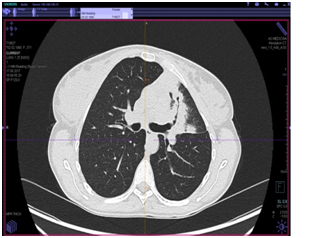
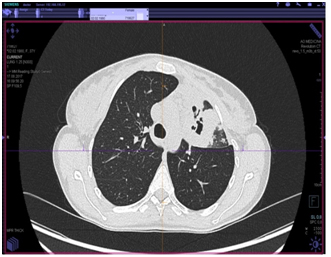
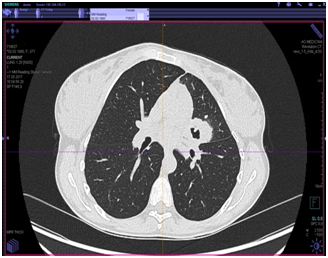
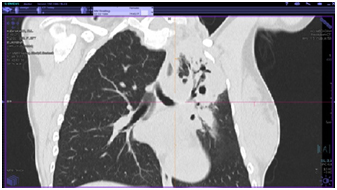
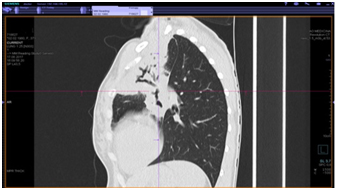
CT scan of the chest organs (from 17.08.2017)
Conclusion: massive infiltrative changes in the upper lobe of the left lung of completely unclear genesis, it is possible that there is both an inflammatory specific nature of the lesion with disintegration and a complication of pneumonia with the formation of an abscess, a malignant process with disintegration is unlikely.
Additionally, a study was carried out (August 26, 2017).
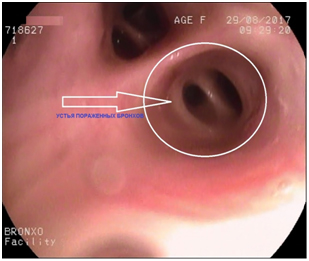
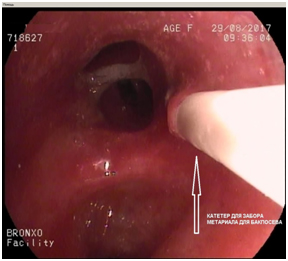
Protocol of endoscopic examination (from 29.08.2017).
Conclusion: no pathological changes in the tracheobronchial tree, accessible to the diameter of the apparatus, were revealed at the time of examination.
Control X-ray of the lungs after bronchoscopy (from 29.08.2017).
Conclusion: left-sided tension pneumothorax.
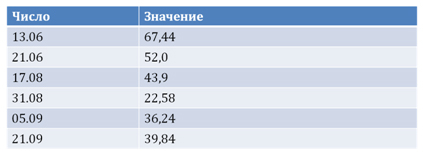
C-reactive protein (mg / l).
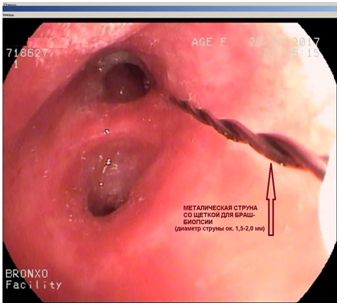
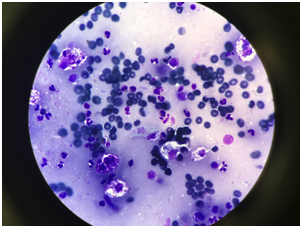
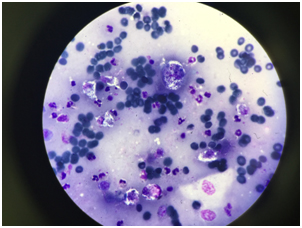
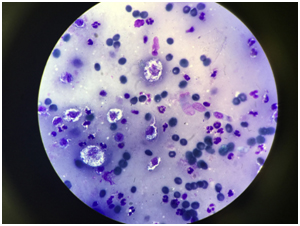
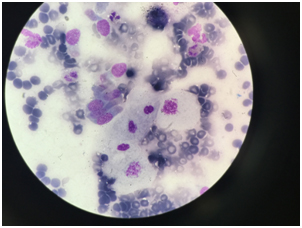
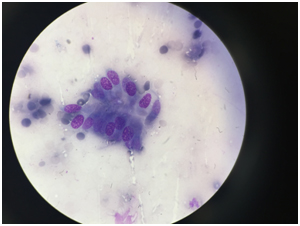
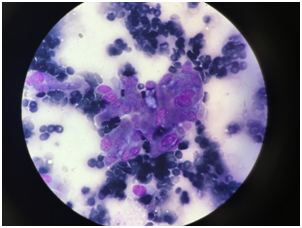
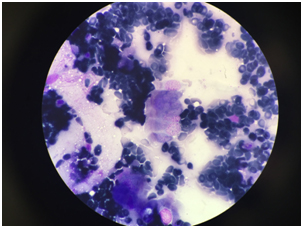
Cytological examination.
Brush biopsy from the left upper lobe bronchus. In the material studied, against the background of erythrocytes, many destroyed cellular elements and a large number of polysegmented granulocytes and alveolar macrophages, separately located and in small clusters, cylindrical cells of bronchial epithelium with signs of proliferation and pronounced reactive changes were found; squamous metaplasia is noted. Cytogram of pronounced nonspecific inflammation.
«Central Research Institute of Tuberculosis»
Diagnosis at admission: Conglomerate tuberculoma of the upper lobe of the left lung in the phase of decay, MBT (-).
Final diagnosis:
Cancer of the upper lobe of the left lung.
Condition after upper lobectomy of the left lung on October 18, 2017